- HOME
- Department
- Respiratory Surgery
Respiratory Surgery

Overview
Respiratory Surgery provides medical care for not only neoplastic diseases such as primary lung cancer, metastatic lung tumor, mediastinal tumor, and malignant pleural mesothelioma but also diseases that require urgent procedures such as spontaneous pneumothorax, empyema, lung abscess, and chest trauma.
Treatment system:Respiratory Surgery mainly performs surgery and currently treats patients with a system of three respiratory surgeons (as of February 2025). The treatment strategy for lung cancer is determined in cooperation with Respiratory Medicine.
Our department actively incorporates robotic technology to conduct surgery with less damage and postoperative management with less pain. We actively provide rehabilitation from the early postoperative stage in cooperation with Rehabilitation to prevent postoperative complications such as pneumonia and pulmonary thromboembolism.
Latest treatment:With recent advances in chemotherapy and immunotherapy, preoperative chemotherapy is performed for unresectable advanced lung cancer, and if it is effective, complete resection (radical operation) is performed.
Postoperative additional treatment:Regarding additional treatment after surgery for lung cancer, postoperative adjuvant chemotherapy will be considered to prevent recurrence based on the Guidelines for Diagnosis and Treatment of Lung Cancer/Malignant Pleural Mesothelioma/Thymic Tumor. There are various methods of administering anticancer drugs such as oral drugs in outpatient settings and drip infusion; the method will be determined based on the progression of lung cancer (stage), type of lung cancer (histological type), and information on genetic mutations.
Radiation therapy:If radiation therapy is necessary after surgery, stereotactic body radiation therapy (SBRT) or intensity modulated radiation therapy (IMRT) is used by Radiology to intensively irradiate tumor while suppressing the exposure to normal tissues. High-precision treatment will be provided for brain metastasis at the Gamma Knife Center.
Main target diseases and treatment
- Primary lung cancer
- Mediastinal tumor (thymoma, thymic cancer, germinoma, cystic tumor [congenital cyst], or neurogenic tumor)
- Pneumothorax
- Empyema
- Pleural tumor (malignant pleural mesothelioma or solitary fibrous tumor)
- Chest trauma
1.Primary lung cancer
Previously, central-type lung cancer associated with heavy smoking was common (tumor develops in the central airway, often squamous cell carcinoma). It was characterized by bloody sputum or atelectasis and pneumonia associated with bronchial obstruction. In recent years, peripheral adenocarcinoma that is asymptomatic and detected by a health checkup and chest X-ray or CT has been increasing.
The indications for surgery are a non-small-cell lung cancer that is at stage 0 to part of stage IIIA, based on the guidelines. Even if a patient has brain metastasis, surgery may be performed while providing treatment for brain metastasis with a gamma knife if the metastasis is limited to a small number of distant metastases (up to five in principle) of a single organ. Stage-I localized small-cell lung cancer is indicated for surgery, but it is very rare.
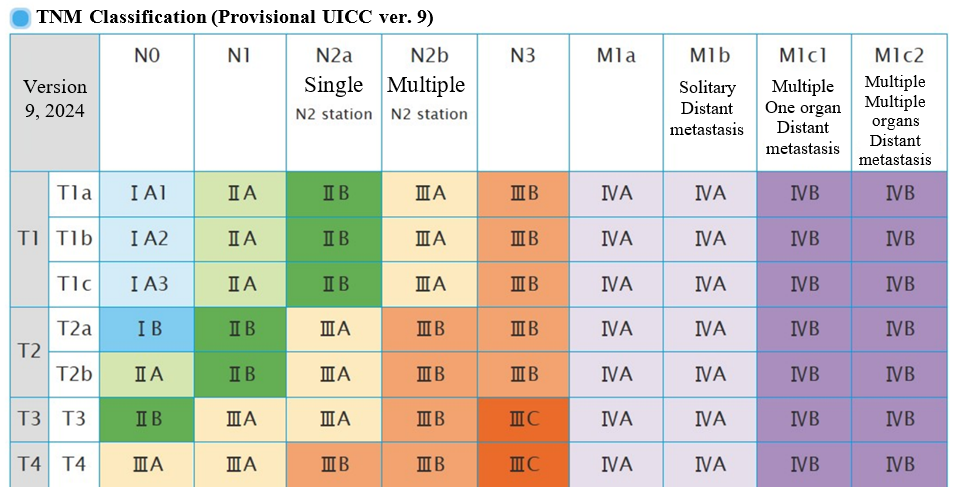
(Source: Pathology and Clinical Medicine Classification of Lung Cancer ver. 9)
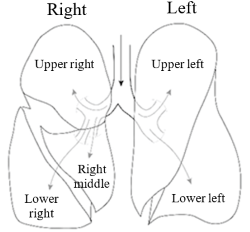
【Anatomy of the lung】
Anatomically, the left lung has two parts, and the right lung has three parts, which consist of a unit called a lobe. There are wrinkles between lobes, which are called fissures. The lobes may be completely separated due to deep wrinkles, but there may be no wrinkles at all. When resecting the pulmonary lobe, it is necessary to resect the dominant blood vessel (pulmonary artery and pulmonary vein) and bronchus (lobar bronchus) to divide the fused fissures (wrinkles).
【Changes in the approach to surgery (from thoracotomy to thoracoscopy and even minimally invasive robotic surgery)】
■Thoracic approach
Before 1990, lobectomy and pneumonectomy were often performed, and the approach was mainly thoracotomy. An 8–30-cm skin incision is made on the lateral thoracic region on the side of the thoracotomy. The muscle is incised, and the place between the ribs is expanded to place a rib retractor. This ensures that the surgeon has the required surgical field for lung resection under direct vision.
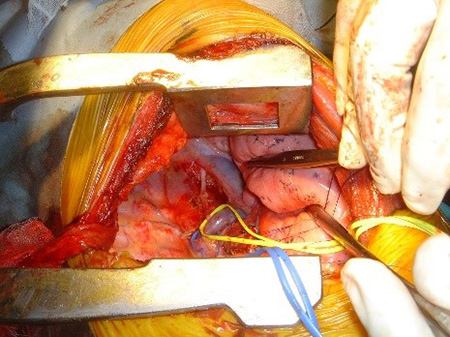
Right lower lobectomy
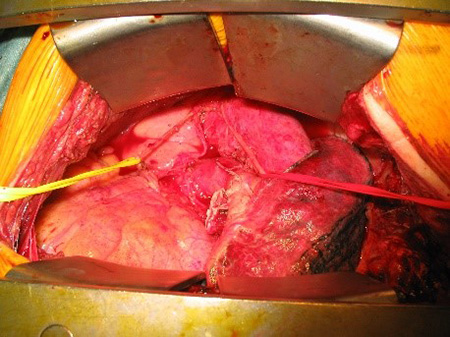
Upper lobectomy
■Thoracoscopic approach

Thoracoscopic surgery started in Japan in the 1990s. In this method, an endoscope is inserted through three to four incisions (port insertion sites) of about 1 cm between the ribs, and surgery is performed while monitoring the image.
An increasing number of institutions have performed more difficult operations such as lobectomy and segmentectomy, as their skills were gradually improved through increased experiences of relatively less difficult operations such as spontaneous pneumothorax. In addition, due to advances in instruments and active efforts of each institution, an increasing number of institutions perform single-port surgery (performed from an incision).
■Robot-assisted approach
According to the revision of medical service fees in 2018, robotic surgery was covered by insurance for a lobectomy for lung malignant tumor and mediastinal tumor. Robotic surgery started to be performed nationwide, and the number of surgical methods covered by insurance increased. Thus, the number of robotic surgeries is increasing.
Surgical method
The standard surgery for lung cancer is lobectomy and systematic lymph node resection (lymph node dissection). The lung lobe where tumor exists is resected, and the mediastinal lymph nodes (N2) are resected, including hilar lymph nodes (N1) and surrounding fat that are likely to cause lymph node metastasis. However, CT screening has become more common, and many early-stage lung cancers are detected. It is a pattern in which cancer grows while replacing the surrounding alveolar epithelial cells, which is expressed as ground-glass pale opacity on CT images (Fig. 1). Since lymph node metastasis is extremely unlikely in such an early-stage lung cancer, surgery is performed without lobectomy. Surgery to reduce the extent of resection includes partial resection at a line sufficiently far from the tumor or segmentectomy in a unit smaller than the lung lobe (Fig. 2. Surgical procedures for partial resection, segmentectomy, and lobectomy).
A recent multicenter study in Japan showed the usefulness of segmentectomy for a lung cancer of 2 cm or less (small lung cancer), and the number of segmentectomy is expected to increase in the future.
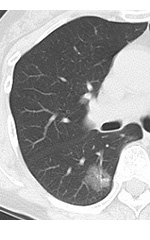
Fig. 1 Early lung adenocarcinoma
Ground glass nodule
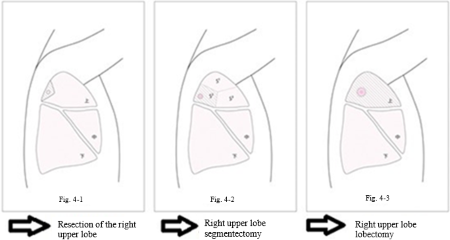
Fig.2 Surgical procedures for partial resection, segmentectomy, and lobectomy
Our approach and procedure for lung cancer
For early-stage lung cancer mainly with ground glass opacity, partial resection and segmentectomy are performed proactively.
At present, partial resection is performed through one incision in principle. If it is necessary to palpate the tumor from a small incision, to confirm the location of the tumor, two incisions may be made. If palpation is difficult, marking (VAL-MAP method) is performed before surgery.
In our department, no thoracotomy is performed for lung cancer with possible lymph node metastasis, advanced lung cancer requiring bronchial angioplasty, or complex segmentectomy. We perform robotic surgery instead. Please refer to the treatment records regarding the characteristics of our department’s robotic surgery and an overview of its results.

Single-port surgery

surgical wound of the single-port surgery
2.Mediastinal tumor
The mediastinum refers to the internal parts of the left and right lungs, excluding the normal structure such as the major cardiac blood vessels, esophagus, and trachea. The mediastinum is divided into four parts: upper mediastinum, anterior mediastinum, middle mediastinum, and posterior mediastinum, and the predilection sites depend on the type of tumor.
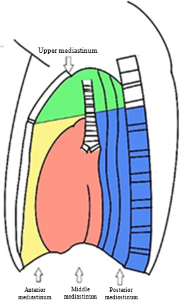
- Upper mediastinal: Neurogenic tumor, thyroid tumor, etc.
- Anterior mediastinum: Thymoma, thymic cancer, thymic neuroendocrine tumor, germ cell tumor, malignant lymphoma, cystic tumor, etc.
- Middle mediastinum: Cystic tumor such as bronchogenic cyst, lymphangioma, etc.
- Posterior mediastinum: Neurogenic tumor, etc.
Typical mediastinal tumor
- Thymoma
- Thymic cancer
- Germ cell tumor, cystic tumor (congenital cyst), and neurogenic tumor
- Robotic surgery for mediastinal tumor (PDF)
3.Pneumothorax
The lungs usually extend in a space called the thoracic cavity surrounded by the ribs, thoracic vertebrae, sternum, and diaphragm, and they move the ribs and diaphragm to breathe.
Pneumothorax is a state involving blowout of the lung. It is caused mainly by a small hole in a balloon-like lesion called a pulmonary cyst (bulla). Symptoms include chest pain caused by the entered air and breathing difficulty when the lung shrinks. It may be cured by rest alone, but if air keeps leaking, the lung will continue to shrink further, making breathing difficult. At this level, a chest tube needs to be placed to release the accumulated air. If an air leak stops, the drain can be removed, and the patient can be discharged. However, if an air leak lasts or a pneumothorax occurs repeatedly, surgery is required. In our department, single-port surgery is performed from an incision of about 2 cm. In a difficult case such as a secondary pneumothorax, we may increase the number to three incisions.
Pneumothorax includes idiopathic pneumothorax (with an unknown cause) and secondary pneumothorax (with some cause).
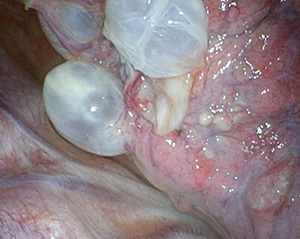
Many bullae at the lung apex
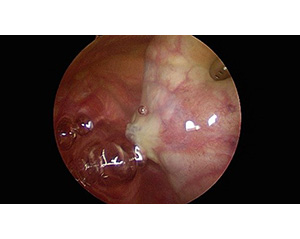
Rupture of a bulla Air leak test
【Idiopathic pneumothorax】
It tends to occur in tall, thin men aged around 20 years. It also occurs in women, although the frequency is low.
【Secondary pneumothorax】
The most common type is a pneumothorax associated with emphysema, which occurs due to bullae caused by the progress in destruction of lung tissues due to smoking.
Typical secondary pneumothorax
4.Empyema
Empyema is a disease in which pus accumulates in the chest due to bacterial infection (pneumonia) of the lung.
5.Pleural tumor
6.Chest trauma
The most common chest trauma includes rib fracture, pneumothorax, and hemothorax caused by a fall.
Rib fractures are generally treated with rest, analgesics, and external fixation with a rib band. Traumatic hemopneumothorax may require drain insertion or, in rare cases, surgery.
If the trauma extends to areas other than the chest, we will comprehensively manage the condition in cooperation with departments in other areas.
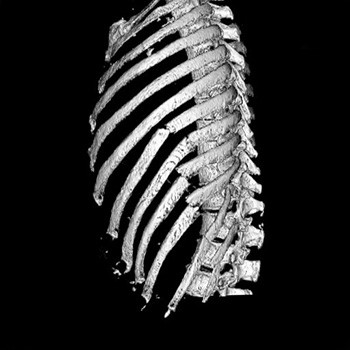
Rib fracture
Message to patients who visit us
Respiratory Surgery strives to provide surgery that can reduce the physical stress of patients by fully using the ability acquired through new technologies and experiences.
We are also actively adopting a variety of new treatment methods. For the selection of treatment methods, we present advantages and disadvantages of each treatment and then ask the patients to select the treatment method that they find reasonable.
Jun Matsumoto, Director